If a patient asks, “Does laser really build collagen, or is it just burning the top layer?”—could you explain the molecular answer?
For decades, we knew lasers made skin look younger. Now, peer-reviewed research has mapped the exact biological cascade: from fibroblast activation to neocollagenesis (the birth of new collagen).
In this post, we break down how laser and light therapies trigger the body’s wound healing cascade, why treatment intervals matter more than the device itself, and what the latest 2024–2026 studies reveal about reversing photoaging at the genetic level.
1. The Cellular Target: The Fibroblast
Collagen doesn’t repair itself. Fibroblasts do.
Fibroblasts are the “construction workers” of the dermis. They synthesize extracellular matrix (ECM) proteins, primarily:
Type I collagen (80–85% of skin’s structure—provides tensile strength)
Type III collagen (10–15%—provides elasticity and reticular structure)
As we age (or accumulate UV damage), fibroblasts become lazy. They downregulate COL1A1 and COL3A1 gene expression and upregulate matrix metalloproteinases (MMPs)—enzymes that shred existing collagen like microscopic scissors .
Key insight: Laser therapy doesn’t “add” collagen. It tricks fibroblasts into resuming youthful repair activity by creating a controlled micro-injury.
2. The Mechanism: From Photons to Collagen Fibrils
Depending on the device, lasers stimulate collagen through one of two distinct pathways:
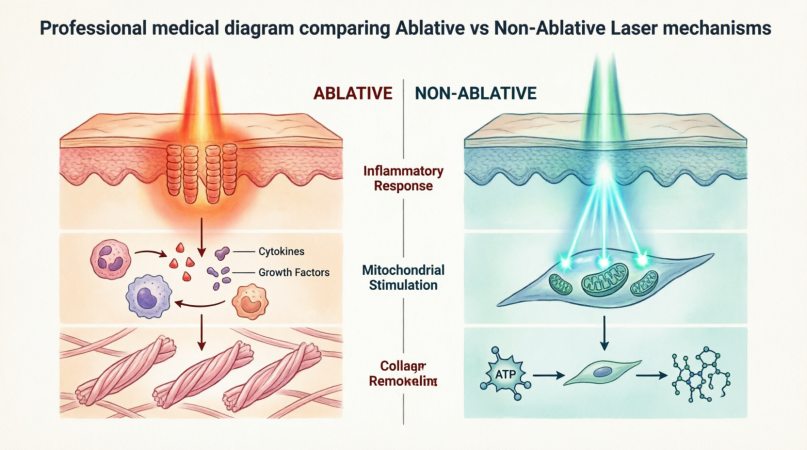
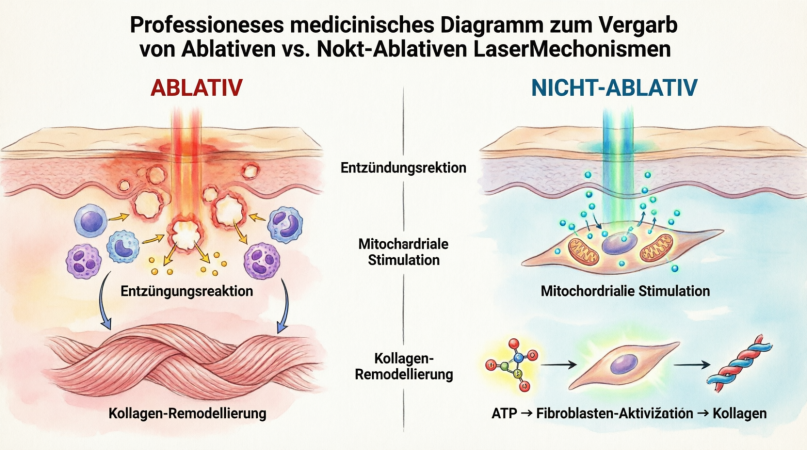
A. Ablative & Fractional Lasers (The “Micro-Wound” Pathway)
Examples: CO₂ (10,600 nm), Er:YAG (2940 nm)
These create microscopic columns of thermal injury (fractional zones). The body responds not as “damage” but as wound healing:
Proliferation (Day 3–14): TGF-β (Transforming Growth Factor-Beta) signaling activates. Fibroblasts migrate to the injury zones.
Remodeling (Week 2–6 months): Neocollagenesis begins. New Type I and III collagen is deposited, organized in parallel bundles (not the haphazard mesh of aged skin).
B. Non-Ablative & Photobiomodulation (The “Metabolic” Pathway)
*Examples: Diode (1440/1927 nm), 675 nm red light, Near-infrared*
These spare the epidermis entirely. Instead of wounding, they use photobiomodulation (PBM) :
Photons are absorbed by cytochrome c oxidase in the mitochondrial electron transport chain.
This increases ATP production and releases nitric oxide.
Result: Upregulation of fibroblast proliferation and collagen synthesis without cell death .
Diagram:A split-diagram comparing Ablative Laser (micro-thermal zones -> wound healing cascade -> new collagen) vs. Non-Ablative Laser (mitochondria -> ATP -> fibroblast activation).
3. Evidence-Based Outcomes: What the Studies Say
The old belief that “laser just burns wrinkles off” is obsolete. Here is what peer-reviewed literature demonstrates:
Collagen Quantification
A 2025 animal study on fractional CO₂ laser found that combining laser with photobiomodulation accelerated dermal regeneration and increased elastic fiber percentage more than laser alone .
Clinical Photoaging Reversal
In a 2024 prospective trial (N=28, Fitzpatrick I-V), a non-ablative fractional diode laser (1440nm + 1927nm) delivered:
96.4% patient satisfaction at 3 months.
Marked improvement in rhytides, skin texture, and radiance (p < .001).
No hyperpigmentation reported in any skin type at the 3-month follow-up .
The Molecular “Switch”
A comprehensive 2026 scoping review in the International Journal of Dermatology confirmed that both ablative and fractional lasers trigger:
Downregulation of MMPs (stopping the destruction of collagen).
Upregulation of COL1A1 and COL3A1 (starting new synthesis).
Crucially, elastogenesis (new elastic fiber formation) is more pronounced after complete ablative procedures .
The Picosecond Revolution
A 2026 study on picosecond laser (755 nm) with diffractive lens array demonstrated something remarkable: photoaging reversal at the molecular level. The laser induced optical breakdown (LIOB) which activated TGF-β/Smad pathways while reducing MMP-9 expression and NF-κB inflammation .
Low-Level Laser Therapy (LLLT)
A meta-analysis aggregating 24 studies found that LLLT had a highly significant overall effect on wound healing (Cohen’s d = +2.22) , with specific augmentation of collagen synthesis (d = +1.80) and reduced healing time (d = +3.24) .
4. The “Secret” of Treatment Intervals
Why do clinics schedule laser sessions 4 to 6 weeks apart? It is not arbitrary—it is biology.
A 2023 bioinformatics study analyzing gene expression in human skin after Er:Glass laser found a two-phase response:
Critical finding: 29 days after the first laser, gene expression was still significantly different from baseline. Treating before 4 weeks interrupts the remodeling phase .
Clinical Rule: Intervals shorter than 4 weeks waste energy. Intervals longer than 8 weeks lose the cumulative “memory” effect of fibroblast stimulation.
5. Wavelength-Specific Effects on Collagen
Not all wavelengths stimulate collagen equally.
Wavelength
Mechanism
Collagen Effect
Best For
675 nm (Red)
Mitochondrial activation
Increases Type III collagen expression (without affecting proliferation)
Prejuvenation, fine lines
980 nm (Near-IR)
Controlled thermal stimulation (50-60°C)
3x increase in dermal thickness; upregulates COL3A1 & FGF2
Skin tightening, remodeling
1440/1927 nm (Diode)
Non-ablative fractional
Significant improvement in rhytides & texture at 3 months
Photoaged skin, all Fitzpatrick types
10,600 nm (CO₂)
Ablative fractional
High COL1A1/COL3A1 expression; durable up to 6 months
Deep rhytides, scars, laxity
6. Clinical Takeaways for Practitioners
If you are designing a collagen-stimulation protocol:
Manage patient expectations: Neocollagenesis takes 90 days to become visible. The “glow” at 2 weeks is edema and re-epithelialization. The real tightening happens at 3-6 months.
Combination is superior: A 2023 study on periocular aging found that fractional CO₂ laser followed by recombinant human collagen infiltration significantly increased skin thickness on ultrasound (P < .001) compared to laser alone .
Dark skin is safe (with the right laser): The 2024 diode laser study included Fitzpatrick V without adverse hyperpigmentation, proving that non-ablative fractional avoids the risks of ablative or IPL in melanin-rich skin .
The Bottom Line
Laser therapy is not cosmetic “smoke and mirrors.” It is controlled mechanobiology. You are using heat or light to reset the dermal transcriptome—turning off inflammatory MMPs and turning on collagen synthesis.
But with great biology comes great responsibility. Misapplied energy (too high fluence, wrong wavelength, inadequate cooling) turns neocollagenesis into necrosis.
Ready to Master the Biology?
Understanding why collagen forms is only half the equation. You also need to know how to select the right device, calculate fluence, and manage adverse events.